Spaull, N. 2020. COVID-19 Policy Brief: Who should go back to school first? Research on Socioeconomic Policy (RESEP). Stellenbosch University.
For the full hyperlinked and formatted version of this policy brief please see HERE.
1. Overview
Risks, transmission rates and costs: The question of when and how children should return to school depends on three main points: (1) Risks to children of illness and death, (2) Transmission of the virus from children to adults and the need to ‘flatten the curve’, and (3) The social and economic costs of keeping children at home. The policy brief below presents evidence on these three issues and argues that when children go back to school the youngest should go back first.
Overview of research on children and COVID-19: The brief presents what appears to be a clear and emerging consensus in the international research literature across all countries[1]: Children aged 0-10 years old are considerably less likely than adults to get infected, either from each other or from adults. They are less likely to transmit the virus, even when they are infected. And it is extremely rare for them to get severely ill or die from COVID-19.
Why the youngest should go back first: In addition to the fact that children 10 years and younger are considerably less likely to get infected, they also present the highest child-care burden to their households. This prevents many parents and caregivers from going back to work and earning an income to support their families. Any response to mitigate the economic disaster from the lockdown and COVID-19 must take account of parent’s additional child-care responsibilities while schools are closed. Secondly, young children are also the least able to follow self-directed learning at home. This is partly because they have not yet learnt to read by themselves, but also because young children simply require higher levels of human interaction and “activity” for them to learn. For most children in South Africa all curricular learning has stopped while schools are closed leading to further inequalities in learning outcomes. Lastly children’s wellbeing increases when they can go to school. Children receive free school meals to supplement their diet, they can interact with their same-age peers, and it gives their caregivers a break from otherwise constant child-care. This improves parents’ mental health and allows them to work, plan and relax, making them better caregivers when children come back from school.
Young children being “locked-up” at home when there are few health benefits to themselves or society is bad for the well-being children, bad for parents and bad for the economy.
Using research to inform policy responses: Judgements about the national threat posed by COVID-19 and mitigation strategies should be informed primarily by advice from virologists and epidemiologists (the author is neither). However, the Department of Basic Education in South Africa, in consultation with these experts, has already decided that schools will now go back (from 1 June 2020), starting with Grade 7 and Grade 12. The current policy-brief argues for a different phasing-in approach to the current one, namely, at the same time that Grade 12 goes back, ECD sites should be opened and Grade R, 1, 2 and 3 should be allowed to return incrementally (rather than Grade 7) using a phased-in approach with special precautions for teachers. This should be combined with close monitoring of infection rates among a random sample of teachers and families of Grade R-3 children. There is a clear rationale for this that is informed by the best available research. Such an approach minimizes the risk to learners and teachers and also allows many parents to go back to work. In short, children should go back to school and the youngest should go back first.
2. International research on COVID-19 and children
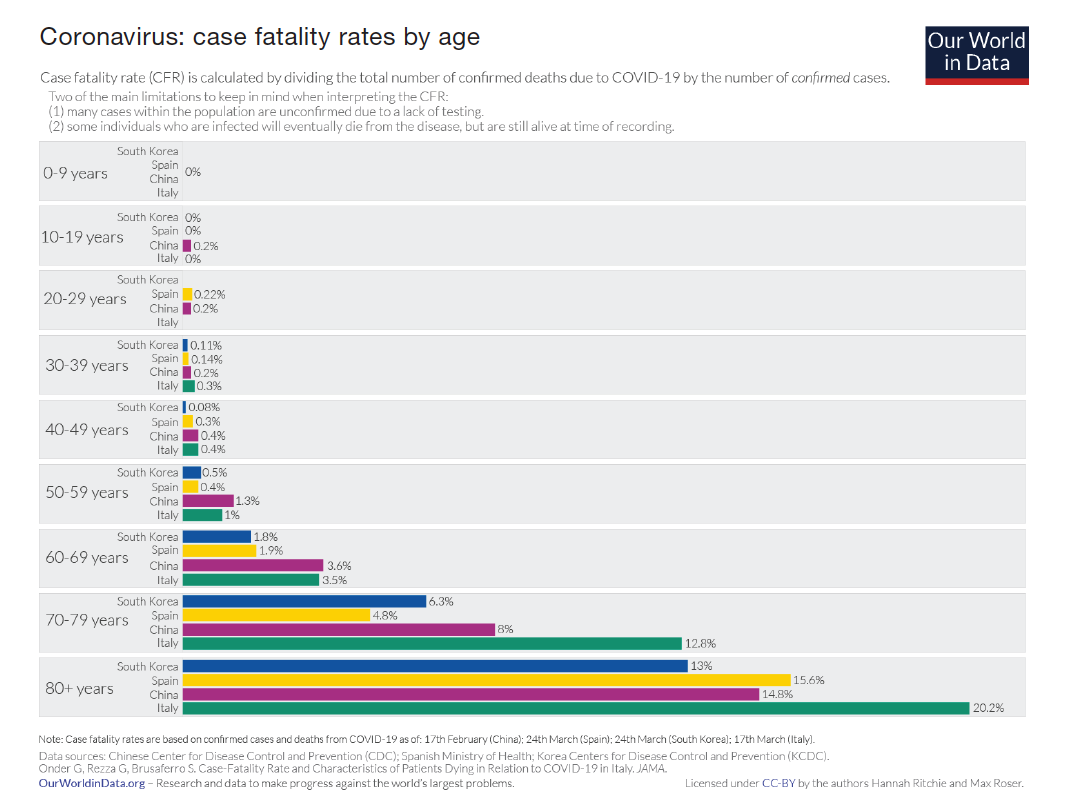
The evidence emerging from countries around the world is clear and consistent: children are less likely to catch COVID-19 and almost never die from it. The graph below shows the fatality rates from COVID-19 by age group for China, Italy, Spain and South Korea. The data reflects all deaths up to 24 March 2020 (Our World in Data, 2020). The clear age bias is evident, with less than 0,3% of fatalities for those less than 40 years of age and “0%” for the 0-9 year-old category.
Included below is a short summary of authoritative research studies reviewing the COVID-19 outbreak in different countries with a special focus on children. To date the best available evidence on whether children can catch and transmit COVID-19 comes from Iceland since they have tested the largest percentage of their population.
Iceland: In their 14 April 2020 article in the New England Journal of Medicine Gudjartsson et al (2020) report that “In the population screening, no child under 10 years of age had a positive result, as compared with 0.8% of those 10 years of age or older.” Even amongst a pre-selected high-risk group that had likely exposure to the virus, children under the age of ten were half as likely to test positive compared to those older than 10.” Furthermore, in an interview with the CEO of the genetic sequencing company working with the Icelandic Directorate of Health to trace all COVID-19 infections they explain that: “Children under 10 are less likely to get infected than adults and if they get infected, they are less likely to get seriously ill. What is interesting is that even if children do get infected, they are less likely to transmit the disease to others than adults. We have not found a single instance of a child infecting parents.”
South Korea: The Korean experience is notable because they were one of the first countries to undertake widespread community testing. In a study looking at the first 7,755 confirmed cases of COVID-19 in Korea, only 1% of cases were among the 0-9 age group (Choe et al 2020). There were no fatalities for any patient under 30 years of age.
Switzerland: In May 2020, the Swiss health ministry’s infectious diseases chief Daniel Koch reported that after wide consultation with clinicians and researchers, “Young children are not infected and do not transmit the virus,” he said. “They just don’t have the receptors to catch the disease.” And went on to say that children under the age of 10 in Switzerland can now hug their grandparents (BBC). This is now the official policy in Switzerland and has subsequently been supported by infectious-diseases paediatricians and the Swiss Pediatric Society (RTS, 1 May 2020).
America: On 1 May 2020 the CDC in America reported that of 37,308 deaths from COVID-19 in America, only 9 (0.02%) were among children aged 0-14 years.
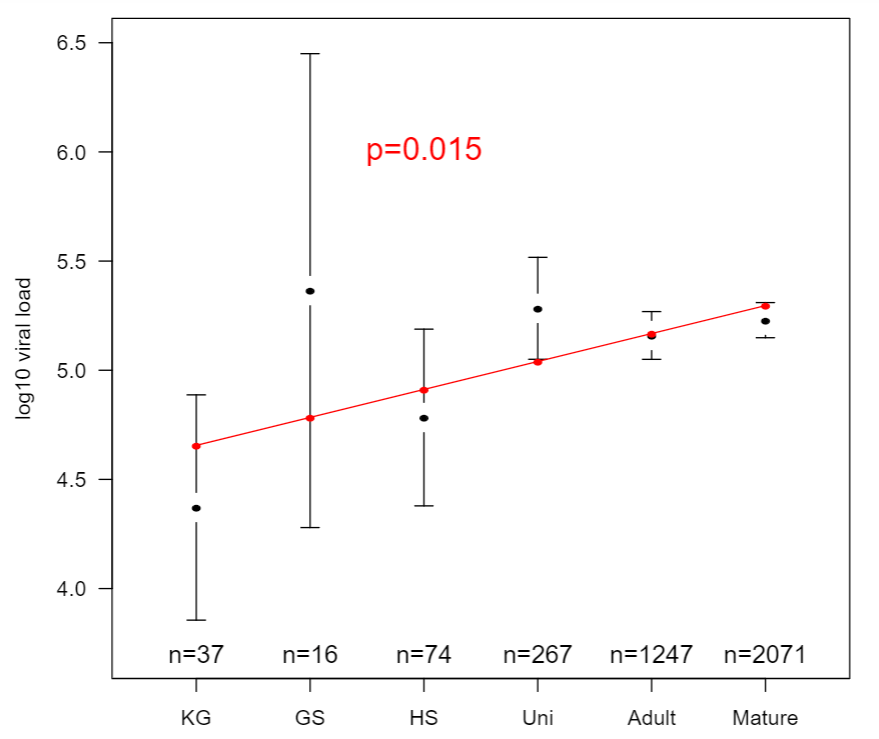
Germany: One German study showed that the children who tested positive for COVID-19 harbour just as much of the virus as adults (Drosten et al. 2020). This has led to speculation that children are as infectious as adults. However, a number of other recently published studies refute this. Studies that look at this question specifically (i.e. tracing studies to identify index cases) show that this is not the case. Children are very rarely the source of infection in a household or a population. These tracing studies are consistent with each other and come from America, Australia, China, the Netherlands, Singapore, and South Korea, and all support the hypothesis that children are not the primary spreaders of the virus.
Italy: In the town of Vo in Italy they screened 86% of their population and found that “No infections were detected in either survey in 234 tested children ranging from 0 to 10 years, despite some of them living in the same household as infected people” (Lavezzo et al. 2020, p.5).
Japan: In a study that reviewed the 313 domestically acquired cases in Japan from January to March 2020, Mizumoto et al (2020) found that: “Children are less likely to be diagnosed as cases, and moreover, the risk of disease given exposure among children appears to be low.”
Netherlands: In April 2020, the Dutch National Institute for Public Health and the Environment reported that “children play a small role in the spread of the novel coronavirus. The virus is mainly spread between adults and from adult family members to children. Cases of children infecting each other or children infecting adults are less common.”
There are also a range of synthesis studies which review evidence across a number of countries and studies. These help to draw out the similarities and differences across these studies. A review of 67 studies on COVID-19 and children concluded that “The role of children in transmission is unclear, but it seems likely they do not play a significant role” (DFTB, 2020: p.8). In a review of 31 household transmission clusters from China, Singapore, the USA, South Korea and Iran, only 3 households (10%) had a child as the index case (Zhu et al, 2020). To put this in perspective, in the H5N1 outbreak, children were the index case in 54% of cases (Zhu et al, 2020). The researchers conclude that “Whilst SARS-CoV-2 can cause mild disease in children, the data available to date suggests that children have not played a substantive role in the intra-household transmission of SARS-CoV-2.”
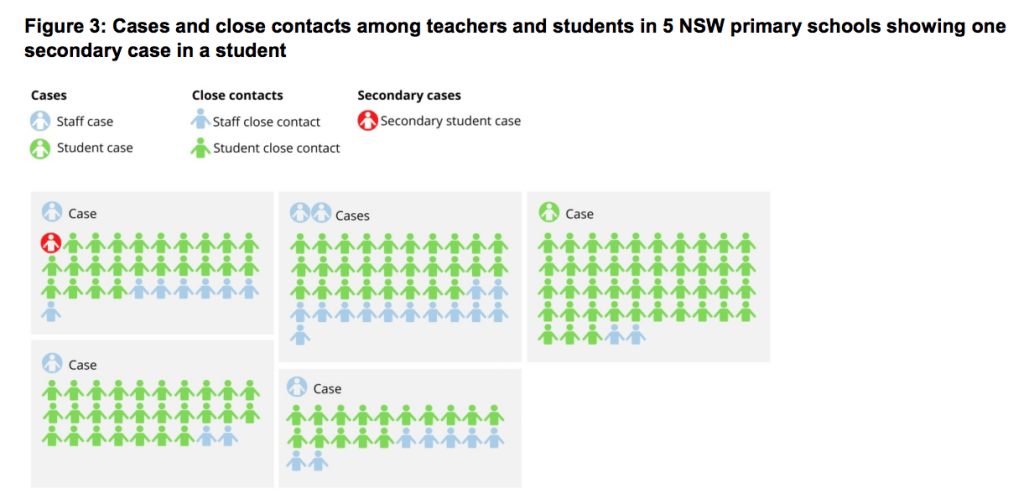
In their April 2020 paper paediatric infectious disease experts Munro & Faust (2020) summarise three recent studies: “A case study of a cluster in the French Alps included a child with COVID-19 who failed to transmit it to any other person, despite exposure to more than a hundred children in different schools and a ski resort (Danis et al., 2020). In New South Wales Australia none of 735 students and 128 staff contracted COVID-19 from nine child and nine adult initial school cases despite close contact (NSW, 2020). In the Netherlands, separate data from primary care and household studies suggests SARS-CoV-2 is mainly spread between adults and from adult family members to children (RIVM, 2020).”
Research emerging across all countries seems to be highly consistent. In brief, children are less likely to get infected (either from each other or from adults) and they are less likely to transmit even where they are infected. The literature on COVID-19 is being rapidly updated as new papers come out. This helpful website summarizes new pediatric COVID-19 literature as it comes out. It is managed by pediatric infectious disease experts Alison Boast, Alasdair Munro and Henry Goldstein. See also this resource from Nature.
3. Are children less susceptible than adults?
Munro (2020) reports that there have been five studies looking specifically at whether children catch the disease at the same rate as adults after they are exposed to a confirmed positive case (an index case). The first study came from Shenzen in China looked at 1286 contacts exposed to 391 positive cases. They found that children caught the disease at the same rate as adults (7.4% for children < 10 years vs population average of 6.6%) (Bi et al, 2020). This finding caused a lot of concern, but four more studies have now been published and all show that children are significantly less likely to get infected compared to adults.
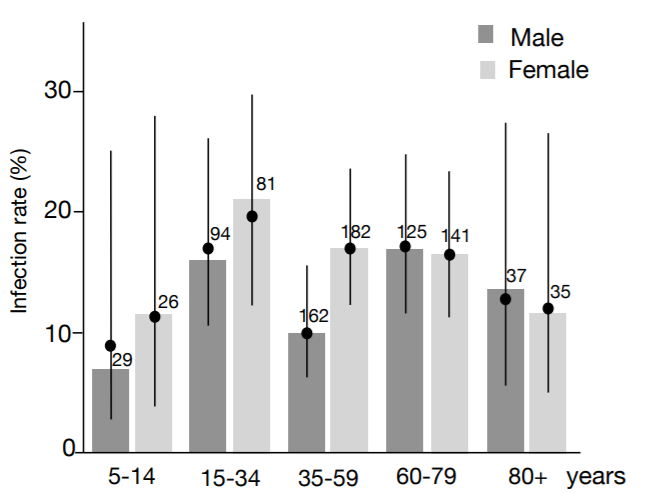
The next study came from Japan and looked at 2496 contacts exposed to 313 positive cases and found children were much less likely to get the disease after exposure. Among children aged 0-19 years who were exposed, 7.2% of boys were infected, and 3.8% of girls were infected compared to 22% of males and females aged 50-59 (Mizumoto et al., 2020).
The third study is from Guangzhou in China which looked at close contacts of 212 positive cases. They found that children were much less likely to get infected (5.3%) compared to adults (12.6%) after exposure (Jing et al., 2020).
The fourth study came from Wuhan in China and looked at 392 contacts exposed to 105 positive cases. They found that only 4% of children (<18) became infected compared to 17% among adults (Li et al., 2020).
The last study comes from Hunan in China which traced 7375 contacts exposed to 136 positive cases. They find that adults aged 15-64 are about four times as likely to get infected compared to those 14 and under (Zhang et al., 2020).
To quote Munro (2020) who summarizes these five studies “In conclusion, we have five studies assessing the secondary attack rate of COVID-19 across age groups, in which four report a considerably lower attack rate in children and one which reports the same in children as the general population. It appears fairly convincing that children are less likely to acquire the infection than adults, by a significant amount.”
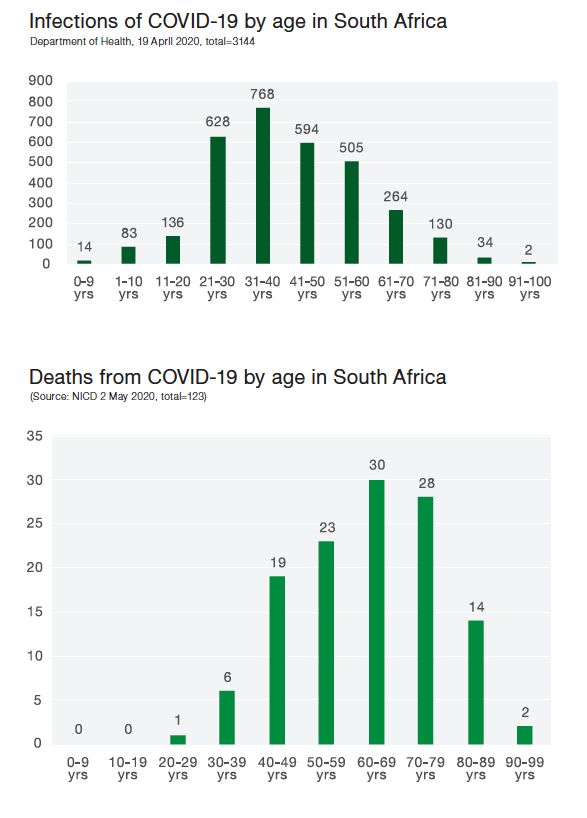
4. Infection rates by age in South Africa
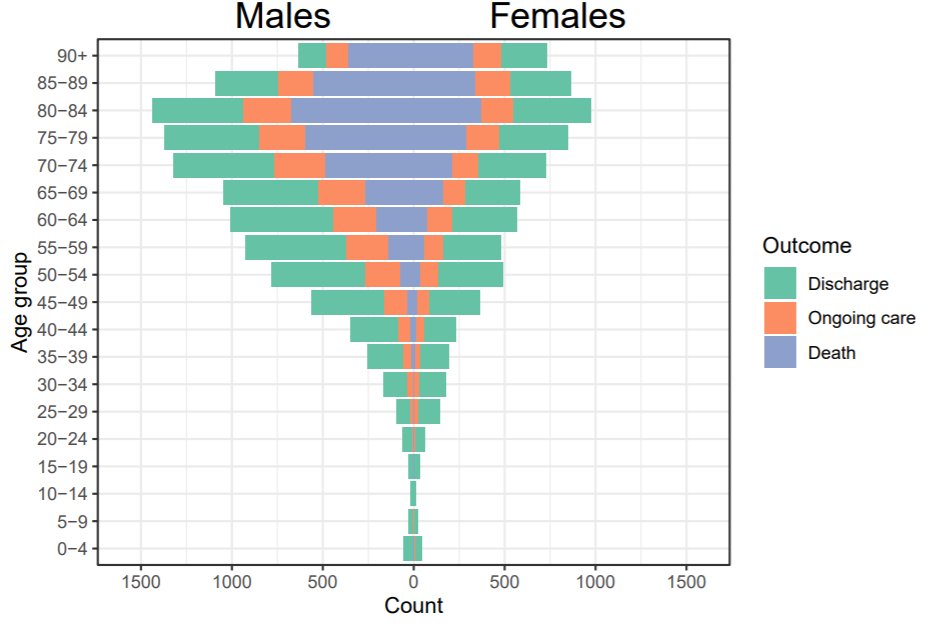
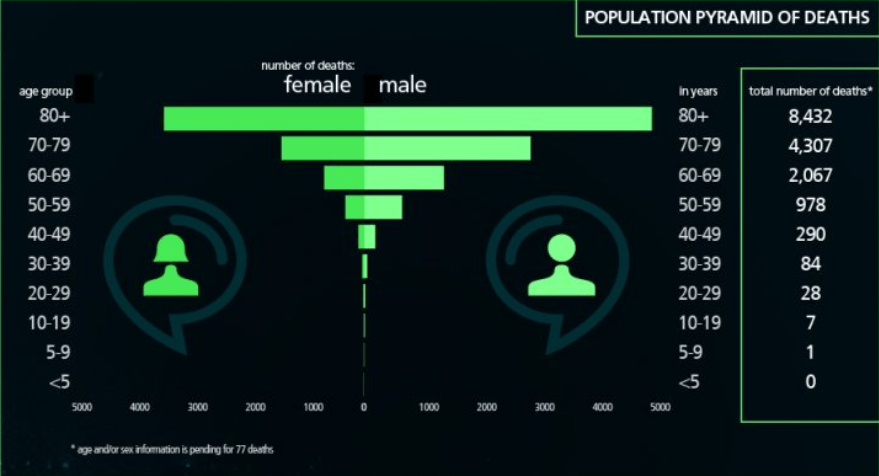
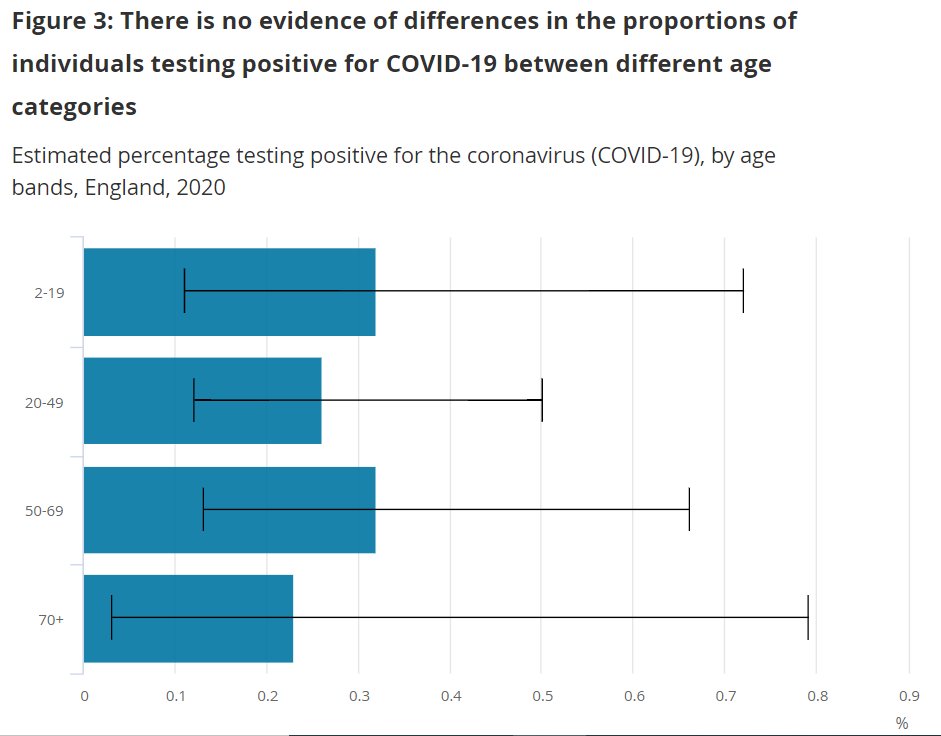
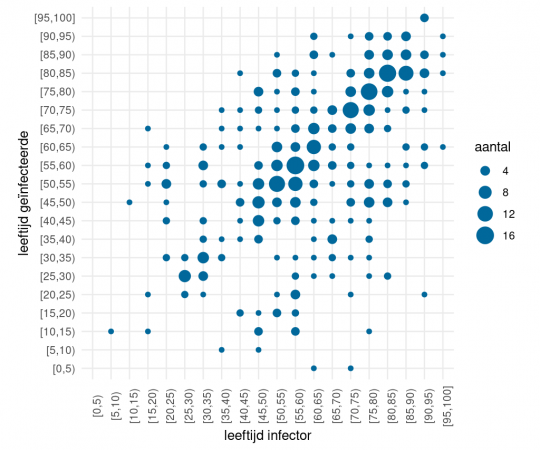
While South Africa has a considerably smaller number of infections and fatalities compared to any of the countries reviewed above, the age-profile of infections and deaths is consistent with the international experience. As of 2 May 2020, 123 people had died of COVID-19 in South Africa but none of these deaths were among those under 20 years of age (NICD, 2020). Of the 3,144 positive cases of COVID-19 in South Africa as at 19 April 2020, only 0,3% were aged 0-10 and 4% were aged 11-20. The two figures below present the full set of data.
5. Do school closures help?
In a widely cited study published in the Lancet Journal of Child and Adolescent Health, Viner et al (2020) conducted a rapid systematic review on the effectiveness of school closures in limiting the spread of COVID-19, They conclude as follows: “Data from the SARS outbreak in mainland China, Hong Kong, and Singapore suggest that school closures did not contribute to the control of the epidemic…Recent modelling studies of COVID-19 predict that school closures alone would prevent only 2–4% of deaths, much less than other social distancing interventions.” In another article, published in Science and also modeling the impacts of different interventions to limit the spread of COVID-19, Zhang et al (2020) use contact surveys of 136 confirmed index cases infected in Wuhan and Shanghai. They conclude that “social distancing alone, as implemented in China during the outbreak, is sufficient to control COVID-19.” Yet they also argue that school closures can help to flatten the curve: “While proactive school closures cannot interrupt transmission on their own, they can reduce peak incidence by 40-60% and delay the epidemic.” It should be noted that while Zhang et al. do consider age-specific susceptibility to infection (p.2), they do not consider age-specific transmissibility or infectiousness (i.e. whether transmission rates are different for different ages). See “Modelling SARS-CoV-2 transmission” in the supplementary materials (p.31) to Zhang (2020) where. A common transmission parameter applies to all ages. If it is true that children are less likely to transmit the virus when infected, which seems likely given the above findings from the literature (also RIVM, 2020) then the assumptions underlying the school closure analysis are incorrect and over-estimate the gains from school closures.
6. Are children continuing to learn at home during lockdown in South Africa?
It is difficult to answer this question definitively but given what we know about learning losses during holiday periods, the lack of access to technology and educational materials at home for the poorest 70% of South African children, and the lack of preparation for distance-learning before the lockdown started, the short answer to this question is no. If one is realistic, for the poorest 80% of learners in South Africa there is virtually no curricular learning that is taking place during lockdown.
Apart from the fact that parents and care-givers are not trained or equipped to teach their own children, the existing lockdown ‘plans’ for learning will not significantly mitigate the losses in learning for children that do not have proper technology-enabled learning at home. At most 5-10% of learners can continue learning at home given their access to computers and the internet. Data from the Trends in International Mathematics and Science Study (TIMSS 2015 Grade 9) shows that for no-fee schools (the poorest 75%), less than half of children in a class have a computer with the internet. Only in the wealthiest 5% of schools do at least 90% of learners have access to a computer and the internet at school (Gustafsson, 2020).
The DBE’s partnership with the south African Broadcasting Corporation (SABC) to provide “COVID-19 Learner Support” via television and radio (DBE, 2020), while admirable, is not a replacement for school. It targets only “Grade 10-12 and ECD” and is only available for 1.5 hours per day across three television channels. Given that these programs would need to be subject and grade specific for them to continue with curricular work, this still amounts to less than 5% of the ‘instruction’ time learners would be receiving if they were in school, assuming they watch all programs dedicated to their grade. It is also not clear what children in Grades R-9 are meant to do.
Access to computers and the internet in South African homes is very low. The General Household Survey of 2018 shows that only 22% of households have a computer in them (StatsSA, 2019: p.63), and only 10% have an internet connection in their home (p.57). While it is true that 90%+ of South African households report access to a mobile phone (p.56), only 60% report access to the internet via their mobile phone. It should further be emphasised that these rates are for adults in the household. One cannot assume that during lockdown children in a household would have exclusive or unlimited access to the cell phone to access educational content. There is also the issue of multiple children in the same household needing to share a mobile-phone, and the high cost of data, although there are now some zero-rated educational sites (Duncan-Williams, 2020).
Given the practical impossibility of continuing with meaningful learning from home – at least for the poorest 80% of learners, the emphasis for the Department of Basic Education should be making schools safe for learners and teachers to return.
7. Conclusion
South Africa’s choice to re-open schools is in-keeping with a number of other countries that have far greater COVID-19 outbreaks and some with shorter lockdown periods. These countries include China, Denmark, Israel, Finland, France, Germany, Japan and the Netherlands. In all cases governments are introducing precautionary measures such as temperature checks, reduced class-sizes, holding classes outside and spacing desks further apart.
Deciding to re-open schools and bring children back in a phased-in approach will involve a number of administrative complexities. These include how to manage the infection risks for adults that facilitate schooling including teachers, principals, administrative staff, transport workers and school feeding employees. Temporarily replacing high-risk individuals such as those older than 60, those with diabetes and other pre-existing conditions etc., will not be simple or easy. Yet this should be held in tension with the severe limitations imposed by school closures; to children’s ability to learn, to care-giver’s ability to earn an income, and to the economy’s ability to function. The economy cannot properly ‘re-open’ while schools are closed. This is especially true for schooling for those 10 years of age and younger who require the most care when at home.
The aim of this policy brief has been to summarize some of the emerging international evidence. The latest evidence suggests that by allowing the youngest children to go back first, policymakers are putting teachers and parents at lower risk than if high-school learners went back to school first. As two pediatric infectious disease experts explain “Severe COVID-19 is as rare as many other serious infection syndromes in children that do not cause schools to be closed” (Munro & Faust: 2020, p.2).
As the Department of Basic Education considers when and how to bring children and teachers back to school, it would be wise to heed the epidemiological evidence emerging from around the world. Younger children are far less likely to catch or transmit the COVID-19 virus and therefore bringing them back to school first is the safest approach – for them, for their teachers, and for the health of our economy and society as a whole.
8. References
Although all references in this brief have been hyperlinked, the full reference list is also provided below.
BBC News. 29 April 2020. Coronavirus: Switzerland says young children can hug grandparents [Online]. Available: https://www.bbc.com/news/world-europe-52470838
Bi, Q., et al. 2020. Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzen, China: a retrospective cohort study. Lancet Infect Dis 2020 April 27.
Boast, A., Munroe, A., Goldstein, H. 2020. An evidence summary of Paediatric COVID-19 literature [Online]. Available: https://dontforgetthebubbles.com/evidence-summary-paediatric-covid-19-literature/
Children and Covid-19. 6 May 2020. National Institute for Public Health
and the Environment, [Online]. Available: https://www.rivm.nl/en/novel-coronavirus-covid-19/children-and-covid-19
Danis, K., Epaulard, O. Bénet, T., Gaymard, A., Campoy, S., Bothelo-Nevers, E., Bouscambert-Duchamp, M., Spaccaferri, G., Ader, F., Mailles, A., Boudalaa, Z., Tolsma, Julien Berra, V., Vaux, S., Forestier, E., Landelle, C., Fougere, E., Thabuis, A., Berthelot, P., Veil, R., Levy-Bruhl, D., Chidiac, C., Lina, B., Coignard, B., Saura, C. 2020. Cluster of coronavirus disease 2019 (Covid-19) in the French Alps, 2020, Clinical Infectious Diseases, dio: https://doi.org/10.1093/cid/ciaa424
DBE. 2020. Basic Education and SABC launch Coronavirus COVID-19 TV and radio curriculum support programmes for learners. (Online). Available: https://www.gov.za/speeches/basic-education-and-sabc%C2%A0launch%C2%A0coronavirus-covid-19-tv-and-radio-curriculum-support [Accessed 7 May 2020]
DFTB. 21 April 2020. DFTB Covid-19 Evidence review [Online]. Available: https://dontforgetthebubbles.com/wp-content/uploads/2020/04/COVID-data-3.pdf
DoH. 2020. Statistics of COVID19 by age and gender. Department of Health. Online. Available: https://twitter.com/healthza/status/1252331290684162048 [Accessed 7 May 2020]
Duncan-Williams, K. 2020. South Africa’s digital divide detrimental to the youth. Mail & Guardian 19 April 2020 (Online): https://mg.co.za/article/2020-04-19-south-africas-digital-divide-detrimental-to-the-youth/ [Accessed 7 May 2020]
Faulconbridge, G. 2020, May 2. UK Could Allow Primary Schools to Reopen as Soon as June 1: Telegraph. New York Times [Online]. Available: https://www.nytimes.com/reuters/2020/05/02/world/europe/02reuters-health-coronavirus-britain-lockdown.html
Gudbjartsson, D.F., Helgason, A., Jonsson, H., Magnusson, O.T., Melsted, P., Norddahl, G.L., Saemundsdottir, J., Sigurdsson, A., Sulem, P., Agustsdottir, A.B. and Eiriksdottir, B., 2020. Spread of SARS-CoV-2 in the Icelandic population. New England Journal of Medicine. DOI: 10.1056/NEJMoa2006100.
Gustafsson, M. 2020 Basic Education the Coronavirus. Department of Basic Education. Pretoria.
Highfield, R. 27 April 2020. Coronavirus: Hunting down Covid-19, Science Museum Group [Online]. Available: https://www.sciencemuseumgroup.org.uk/hunting-down-covid-19/
Jing, Q et al. 2020. Household Secondary Attack Rate of COVID-19 and Associated Determinants. medRxiv preprint doi: https://doi.org/10.1101/2020.04.11.20056010
Li et al., 2020. The characteristics of household transmission of COVID-19. Clinical Infectious Diseases, ciaa450. (Online). Available: https://doi.org/10.1093/cid/ciaa450
Lavezzo, E., Franchin, E., Ciavarella, C., Cuomo-Dannenburg, G., Barzon, L. and Del Vecchio, C., 2020. Suppression of COVID-19 outbreak in the municipality of Vo’. Italy. medRxiv preprint. doi: https://doi. org/10.1101/2020.04, 17.
Mandavilli, A. 2020, May 5. New Studies Add to Evidence that Children May Transmit the Coronavirus. New York Times [Online]. Available: https://www.nytimes.com/2020/05/05/health/coronavirus-children-transmission-school.html
Mizumoto, K., Omori, R. and Nishiura, H., 2020. Age specificity of cases and attack rate of novel coronavirus disease (COVID-19). medRxiv. doi: https://doi.org/10.1101/2020.03.09.20033142
Munro, A. 2020. The missing link? Children and transmission of SARS-CoV-2, Don’t Forget the Bubbles, 2020. Available at: http://doi.org/10.31440/DFTB.25585
Munro, A. P. S., Faust, S. N. 2020, May 5. Children are not COVID-19 super spreaders: time to go back to school. Archives of Disease in Childhood Published Online. doi: 10.1136/archdischild-2020-319474
National Centre for Immunisation Research and Survailance. 26 April 2020. Covid-19 in schools – the experience in NSW [Online]. Available: http://ncirs.org.au/sites/default/files/2020-04/NCIRS%20NSW%20Schools%20COVID_Summary_FINAL%20public_26%20April%202020.pdf
NICD. 2020 COVID-19 Update 2 May 2020. National Institute for Communicable Diseases (NICD). Online. Available: https://www.nicd.ac.za/covid-19-update-46/ [7 May 2020]
Our World in Data. 2020. Case fatality rate for COVID-19 by age. Online. Available:
https://ourworldindata.org/coronavirus#case-fatality-rate-of-covid-19-by-age [7 May 2020]
Provisional Death Counts for Coronavirus Disease (Covid-19). 1 May 2020. Centres for Disease Control and Prevention [Online]. Available: https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm
RTS News. 1 May 2020. Daniel Koch: “Je suis sûr de notre analyse concernant les enfants” [Online]. Available: https://www.rts.ch/info/suisse/11291943-daniel-koch-je-suis-sur-de-notre-analyse-concernant-les-enfants-.html
StatsSA. 2019. General Household Survey 2018. Statistics South Africa. (Online). Available: http://www.statssa.gov.za/publications/P0318/P03182018.pdf. [Accessed: 1 May 2020].
Viner, R.M., Russell, S.J., Croker, H., Packer, J., Ward, J., Stansfield, C., Mytton, O., Bonell, C. and Booy, R., 2020. School closure and management practices during coronavirus outbreaks including COVID-19: a rapid systematic review. The Lancet Child & Adolescent Health, 4(5). DOI: https://doi.org/10.1016/S2352-4642(20)30095-X
Vogel, G., Couzin-Frankel, J. 2020, May 4. Should schools reopen? Kids’ role in pandemic still a mystery. Science [Online]. Available: https://www.sciencemag.org/news/2020/05/should-schools-reopen-kids-role-pandemic-still-mystery#
Williams, D. 2020, May 3. Hope and Havoc as Some Israeli Schools Reopen Under Coronavirus Curbs. New York Times [Online]. Available: https://www.nytimes.com/reuters/2020/05/03/world/middleeast/03reuters-health-coronavirus-israel-schools.html
Zhanget, J. et al., 2020. Changes in contact patterns shape the dynamics of the COVID-19 outbreak in China. Science. Science10.1126/science. Available: https://science.sciencemag.org/content/sci/early/2020/04/28/science.abb8001.full.pdf
Zhu, Y., Bloxham, C.J., Hulme, K.D., Sinclair, J.E., Tong, Z.W.M., Steele, L.E., Noye, E.C., Lu, J., Chew, K.Y., Pickering, J. and Gilks, C., 2020. Children are unlikely to have been the primary source of household SARS-CoV-2 infections. medRxiv. doi: https://doi.org/10.1101/2020.03.26.20044826
[1] The majority of the current research comes from high-income countries (with the exception of China and Iran), mostly because high income countries experienced the outbreak first and the research response has been largest in these countries. They have also conducted the most screening and testing and therefore have the most reliable indicators of transmission.