SA is in flux: we’re waiting for what we know we need, even as we gird ourselves for disappointment. We’re waiting for an uptick in the economy; waiting for jobs; waiting for the ANC to sort out who is suspending who — but most of all, we’re waiting for vaccines.
The latest results of our National Income Dynamics Study — Coronavirus Rapid Mobile Survey (Nids-Cram), released this week, show that in February and March this year, the vast majority of South Africans (71%) said they would take the vaccine if they could. The problem is, there is none available.
By May 4, SA had vaccinated only 353,000 people. This is less than half those vaccinated in Kenya (853,000) or Ghana (850,000), and lower than in poorer countries like Senegal (417,000) or Zimbabwe (452,000). This picture is even more sobering if you consider the population size. Only 0.6% of SA has been vaccinated — less than Iraq (0.8%), Somalia (0.8%), Afghanistan (1%), and Libya (1.2%), and also less than the vaccination rate in 140 other countries.
Why is this? SA has the resources. It has the expertise. It has the health infrastructure. Instead, it would seem, there was a failure to strategically plan, and to hedge bets. Given the uncertainty around new vaccines, many countries sourced multiple types in the hope that at least one would work. SA came late to that party, then put all the eggs in the AstraZeneca basket — which proved less effective against the local variant. So here we are, back to square one.
Fingers crossed, May could be a turning point. Health minister Zweli Mkhize says SA will get 6-million Pfizer-BioNTech vaccines and 1-million Johnson & Johnson vaccines this month. And President Cyril Ramaphosa says the government has bought vaccines to cover more than 40-million people. All these vaccines, we are told, will arrive at some point in 2021. However, Ramaphosa hasn’t given specifics. So when those vaccines actually arrive, and how quickly they’re administered, remains to be seen. All while a third wave of Covid threatens to break.
Vaccine hesitancy
While SA has been preoccupied with supply problems (how to get more vaccines), it will, like other countries, soon confront a demand problem: how do we get people to take the jabs we do have? Today, the US has vaccinated about 150-million people (45% of its population), but the average number getting a first or single dose has fallen by nearly 50% since April 13.
That was the day that US health officials announced they would temporarily stop the rollout of the Johnson & Johnson (J&J) vaccine, because a tiny proportion of people getting the vaccine had developed blood clots.
This was a huge failure of judgment by the US — and by SA, which slavishly followed that approach. The US had other vaccines to offer, while SA simply paused its entire rollout without any other alternative. Among 7-million US adults vaccinated with the J&J jab, six people (0.00009%) developed blood clots. One died. Oxford researchers have shown that you are 8-10 times more likely to get a blood clot if you get Covid than from the vaccine, and 3,000-times more likely to get a blood clot from birth control pills (a 0.3% chance).
While regulators said they pressed pause due to “an abundance of caution”, it was a failure of judgment on multiple levels. SA (unlike the US) had no other vaccine at the time. The US stopped J&J, but continued with Pfizer and Moderna — but SA stopped rolling out the only vaccine it had. Apart from the fact that the mortality risk from Covid is orders of magnitude greater than the infinitesimal risk of blood clots, it means South Africans will have died unnecessarily due to that pause. But there is another more insidious cost: the increase in vaccine hesitancy, since people are now more wary of the vaccine.
Few genuinely understand that you are as likely to get struck by lightning (one chance in a million) as you are to get a blood clot from a vaccine. It’s not going to happen — but thousands of people who were on the fence may now opt against vaccination. The latest Nids-Cram (wave 4) results, released this week, shed light on whether these communication blunders are likely to have an impact on SA’s rollout. While the survey showed that 71% of South Africans are willing to get a vaccine (higher than many countries), the flip side is that nearly a third were vaccine hesitant. The three main reasons for hesitancy were: concern about side effects (31%); lack of belief in effectiveness (21%); or general lack of trust in vaccines (18%). To combat vaccine hesitancy, we need to know not only why people are hesitant, but also who they are.
This new data shows that those most at risk of Covid (the elderly and those with chronic conditions) are more willing to get the jab. By contrast, those least at risk — people aged between 18 and 25 — were less willing, with only 63% saying they would have a vaccination. This isn’t entirely surprising. As research has revealed elsewhere, those who trust social media as an information source (predominantly young people) were significantly more likely to be vaccine hesitant. One unexpected finding from the survey results was that a respondent’s home language was also a significant predictor of vaccine hesitancy, with 42% of Afrikaans home-language respondents being vaccine hesitant. This is higher than the national average of 29% and far higher than in people belonging to seven of the 11 language groups.
Though Nids-Cram is not provincially representative, in light of the predominance of Afrikaans in the Western Cape and Northern Cape, it accords with the finding that people from these provinces had higher vaccine hesitancy rates of 42% and 41%. More research is needed to understand this finding. But it is a key insight because vaccines are being rolled out provincially and the media that reaches them is predominantly segmented by language.
To what extent have the communication blunders affected these figures? It must be said that already in the Nids-Cram data in February and March, high rates of hesitancy were observed among certain groups — even before the temporary pause of the J&J rollout. However, this past weekend Gauteng premier David Makhura revealed that the J&J suspension did seem to be affecting vaccine registrations in his province. In the past three weeks, of the 1.3-million Gauteng residents older than 60, only 235,000 (18%) had registered to get a vaccine.
It shows there is no room for fuzzy messaging around the efficacy and safety of the jab, if we want a successful roll-out. But the bungle around the J&J vaccine points to what I believe is a bigger underlying problem: politicians are slavishly following the recommendations made by medical experts and trying to minimise deaths, rather than weighing up all sources of harm. Mkhize’s Ministerial Advisory Committee (MAC) is currently made up of 51 doctors and medical academics, but not a single social scientist. Perhaps if there were people from the social sciences (like communications experts, economists and sociologists), the J&J debacle wouldn’t have happened.
Of course, it is a welcome change that the president and his health minister are listening to medical experts — a notable change from the Mbeki or Zuma eras, when Aids denialism was rampant — but we mustn’t fall off the horse on the other side. Medical experts are trained to measure medical risks, and make judgment calls about the efficacy of trials and rates of transmission. But a vaccinologist will be the first to admit he or she knows little of the non-medical risks like increasing unemployment, rising hunger, and growing learning losses. Measuring the social and economic costs of a nationwide lockdown isn’t part of a vaccinologist’s expertise. Instead, it is the politicians’ job to make the call as to what the right course of action is, when it comes to lockdowns, or opening schools.
Take schooling. Medical experts say the social distancing guideline to prevent the spread of Covid should be 1m-2m. Education officials reply that classrooms were not designed to have such large spaces between children — so if we need that distancing, we need “rotational timetables”, where only 50% of children can attend school on any one day. Last year, SA’s National Coronavirus Command Council accepted the experts’ distancing advice for schools without question, leading to rotational timetables in almost all no-fee schools, which make up more than 70% of the country’s schools. But how does one measure the costs of 5-million children not attending school on any one day for an entire year, or two?
Do the hypothesised benefits of limiting the spread of Covid justify these long-term costs to children? That’s not a decision for the medical experts, but for politicians — who are elected to use their judgment about what is in their population’s best interests, by weighing up the costs and benefits. Let’s consider these nonmedical costs.
Learning losses and school feeding
The rotational timetables that have been implemented in no-fee schools have created two major problems. The first is a loss of school days and learning; and the second is the loss of school meals, since poorer children generally don’t get meals on days they don’t go to school. The phased re-opening of public schools and implementation of rotation timetables means that in 2020, primary school learners lost 60% of a possible 198 school days.
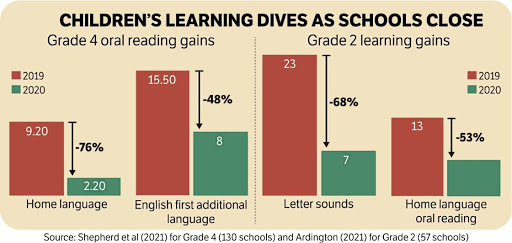
For the first time since the pandemic started, we now also have data on learning outcomes for children affected by the pandemic. This makes it possible to estimate the true educational costs of lost schooling. In a paper published this week, Debra Shepherd and her co-authors examine these learning losses. This research was possible because the department of basic education, together with independent researchers, collected new data from two studies of 130 no-fee primary schools in Mpumalanga, and 57 no-fee primary schools in the Eastern Cape.
By comparing learning gains in 2020 against 2019, researchers estimated the impact of Covid and rotational timetables in no-fee schools in grade 2 and grade 4. The results confirm the worst fears: primary school children in these no-fee schools learnt 50%-75% less in 2020 than normal. Put differently, grade 4 learners in 2020 learnt a quarter of what their peers learnt in 2019.
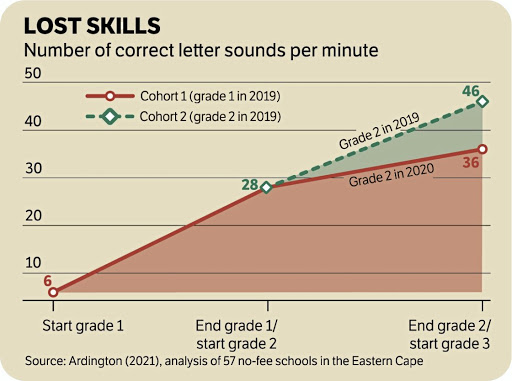
This is all the more disturbing since education is a cumulative process, where subsequent learning depends on prior learning. Using that same data, we can compare the learning trajectories of children who were in grade 1 in 2019 and see how they fare in grade 2 in 2020. The graph shows how the learning trajectory of those children affected by school closures and rotational timetables flattened in 2020. The impact is likely to be felt for years to come, with some suggesting we will be able to get back to pre-pandemic learning outcomes only by 2030.
And schools are about more than learning. In 2019 it was estimated that 9-million learners benefited from free school meals. The Nids-Cram survey asked respondents with children at school if their child had received a school meal in the previous seven days. For the dates that schools were open in February and March this year, less than half (43%) said their child had had a meal in the previous seven days. This suggests the feeding programme still hasn’t recovered — it is well below the pre-pandemic level of 65% in 2018 — and the main reason is the rotational timetable. Given the extraordinarily high costs that children are paying, educationally and nutritionally, because of rotational timetables, it is unsurprising that most parents and caregivers support the full re-opening of schools. In November 2020, Nids-Cram respondents with children in their households were asked: “Do you think children should be able to attend school every day?” In all, 58% answered yes. Given all the evidence, it’s unclear why SA still practises rotational timetables.
Risks to learners and teachers
At the start of the pandemic, when there was still so much uncertainty, closing schools was a rational and justified response. We didn’t know if children caught and spread the virus like adults, or if they were at severe risk from Covid.We know now. The risks to children of getting ill or dying from Covid are exceedingly low. To date, 194 children aged between five and 19 have died of Covid in SA — 0.4% of the total 51,527 deaths. For perspective, Stats SA estimates that of those aged between five and 19, about 12,870 die of “regular” causes in a given year. The issue, of course, is that it’s not only children who are at risk if schools increase transmission — there are also teachers and parents to consider.
Again, we have more evidence now than we had last year. In January, the National Institute for Communicable Diseases (NICD) released a report revealing “no consistent changes in incidence trends, associated with the timing of opening or closing of schools”.
But that’s for the general population — what about teachers specifically? In a report released this week, professor Martin Gustafsson analysed the department of basic education’s national teacher payroll database (Persal) for 2020, to calculate the number of excess teacher deaths from Covid compared to 2019. This is an incredibly accurate source of information on teacher mortality. When teachers die, they are removed from the payroll database. The analysis showed that these “excess deaths” map almost perfectly onto the first and second “waves” of the pandemic (see graph above), indicating they are almost certainly related to Covid. (The slight difference between the red and black lines is due to the delay in reporting national deaths since payroll data is less delayed.) Critically, however, this study reveals that there is no discernible relationship between teacher deaths and when schools are open.
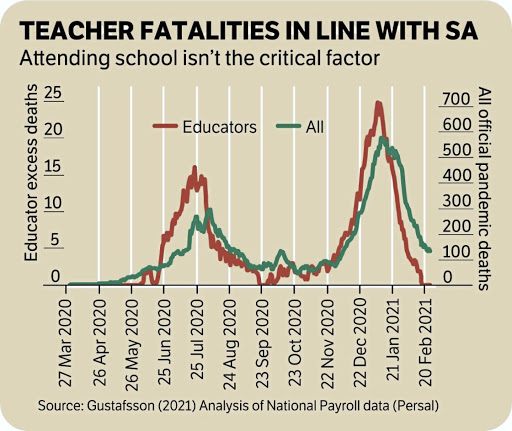
Of the 401,327 teachers on the payroll, 1,678 are estimated to have died from Covid between the end of March 2020 and the end of February 2021. While tragic, it reveals that most “excess teacher deaths” occurred when schools were closed. We don’t see substantial excess deaths among teachers between September and November 2020 — when all grades were attending school. The SA Medical Research Council estimates that SA’s total excess deaths up to January 23 was 125,744. So, excess teacher deaths make up 1.3% of total excess deaths, with the other 98.7% coming from other fields of work and the unemployed. The analysis also shows that teachers at secondary schools are not at higher risk of Covid transmission than teachers at primary schools. This supports the claim that schools are not the main cause of Covid infection among teachers.
Vaccinate like our lives depend on it
According to Mkhize, SA will enter phase 2 of the vaccination strategy on May 17. The plan is to have 40-million people aged 18 years and older vaccinated by February 2022 — all using Johnson & Johnson and Pfizer-BioNTech vaccines.
To reach that goal, SA needs to administer 188,000 doses a day, every day, for the next 287 days. Yet in the past three months we administered only 353,000 shots. Granted, these were part of the Sisonke trial of health-care workers. But if you do the maths regarding the envisioned rollout rate, this would make SA the world leader in vaccine administration — faster than Chile, the UK or Israel, the three fastest countries to date.
The world leader, Chile, managed “only” 117,000 a day for 132 days. So SA — which now ranks 140th in the world in administering jabs — will have to vaccinate faster than the fastest countries in the world. Most experts I speak to know this is not possible, which is why the thinking has shifted from herd immunity to epidemic control. Covid, like the flu, will be with us for the foreseeable future, with top-up shots to protect against new variants.
The strategy will centre on vaccinating (and re-vaccinating) the elderly and those at high risk. This is still a mammoth task akin to the roll-out of antiretrovirals at the peak of the HIV/Aids epidemic. The government needs to vaccinate like our lives depend on it. But we also need to accept that we are entering a new normal where schools are fully open, and children and teachers wear masks. If we continue to deny children 50% of their education, we are moving closer to the reality of writing off a generation of children, the lost “Covid kids”.
The human and financial costs associated with lockdowns, and an uncontrolled pandemic, are thousands of times higher than any conceivable costs of getting and distributing vaccines. This is why every other country has thrown everything they have at this.
Less than a decade ago, SA went from the country with the highest uncontrolled spread of HIV in the world, to the country with the largest antiretroviral programme. It was thanks to a system-wide urgency, and partnerships between the government, the private sector and donors. And it was only possible because it was treated as a war effort, prioritised above all else.
This is what SA needs to do again.
//
This article was first published in the Financial Mail on the 12th of May 2021.
For the full NIDS-CRAM Wave 4 Synthesis Report see here. For the full list of papers see here: